

Hemorrhoid Care Rubber Band Ligation Using the CRH O’Regan System™
Successfully Integrate Techniques Into Your Practice, Benefitting Your Patients and Your EASC
BY MITCHEL GUTTENPLAN, MD FACS – DAVID A. JOHNSON, MD FACP, FACG, FASGE – BERGEIN F. OVERHOLT, MD, MACG, FACP, FASGE
Symptomatic hemorrhoids are a very common problem, affecting as many as 50% of the population by the time they reach the age of 50. Most gastroenterologists (as well as other physicians) have historically deferred definitive treatment of these patients for reasons stated below. Recently, however, there has been widespread and enthusiastic support/embracement of a definitive hemorrhoidal banding technology which is safe, effective, and easy to use. CRH Medical Corporation (CRH) in Vancouver, BC, Canada, has developed a comprehensive training and support program to accompany its CRH O’Regan System™ (fig. 1), a simple, singleuse, disposable, suctionbased hemorrhoid rubber band ligation technology. A description of the technique, training and support program, as well as the benefit to the GI’s patients and practice are provided. The incorporation of this technology into the gastroenterology standard practice has an obvious rationale for an expanded quality of patient care, but also an extremely favorable alternative revenue stream, as well as a source of new patients for the practice.
THE OPPORTUNITY
Symptomatic hemorrhoids are a very common problem, as it has been estimated that 50% of the population will have significant problems by the time they reach 50 years of age, and the prevalence rate has been stated as being over 4%1. The exact number of patients suffering from hemorrhoids is unknown, as it is generally accepted that only a small minority actually seek care for their disorder rather than rely solely upon “over the-counter” remedies. However, the National Center for Hemorrhoid Care Health Statistics states that as may as 23 million people have symptoms from internal hemorrhoids 2,3. Many gastroenterologists (and others) have tended to shy away from definitive treatment (non-pharmocologic) for the vast majority of these patients, in large part because of the reputation of surgical hemorrhoidectomy (pain, disability, prolonged recovery), as well as the difficulty, expense and sometimes uneven results of many of the other mechanical non-surgical options available. Additionally, many GI fellowship programs do not spend much time dedicated to training their fellows in the diagnosis and treatment of hemorrhoids and other ano-rectal disorders, adding to this hesitancy. The combination of these factors—a common problem which many clinicians avoid treating—has led to a large yet dramatically underserved group of patients that can benefit greatly from your care. Expanding the scope of your practice by caring for hemorrhoids and other ano-rectal issues presents a tremendous opportunity for your patients and your practice.
Figure 1 The CRH O’Regan System™, courtesy CRH Medical, Vancouver, BC, Canada

NON-SURGICAL OPTIONS FOR HEMORRHOID CARE
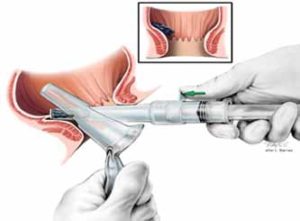
There are several outpatient, nonsurgical techniques used in the care of hemorrhoids, including Infrared Coagulation (IRC), sclerotherapy, microelectric current desiccation, bipolar cautery, heater probe cautery and Rubber Band Ligation (RBL). RBL was first described by Blaisdell in 1954 and modified by Dr. Barron in 19634, 5. It is now among the most frequently used nonsurgical methods in the treatment of symptomatic hemorrhoids. RBL works by causing ischemic necrosis of a portion of the hemorrhoidal tissue and the resulting submucosal fibrotic and inflammatory reaction, effectively “pexing” the redundant mucosa to the underlying muscular layer. This “fixation” of the tissue then eliminates the mucosal prolapse that is at the core of the problem in these patients. These treatments are suitable for symptomatic patients that have been refractory to medical management, and can easily be done in an Ambulatory Surgical Center (ASC) or even in the office setting with no pre-procedure preparation or sedation required. There exist several RBL devices in the marketplace, including the CRH O’Regan System™ which is a singleuse, totally disposable, syringe-type suction ligator that allows for the quick, safe, effective treatment of patients with hemorrhoids utilizing a technique that takes less than a minute to perform. The technology is unique in that it requires no “wall suction,” while offering a “single-handed” approach that may be used with or without an anoscope (fig. 2, 3). The efficiencies offered by the technology and techniques afford for an extremely efficient patient flow, a minimal need for medical assistance, and the procedure can be easily performed in an ASC or clinic setting with virtually no capital expenditure required. The technique involves the introduction of the CRH O’Regan System™ through the anus, directing it towards the hemorrhoidal column to be treated. The tissue is drawn up into the syringe, confirmation of placement is made by twisting the engaged bander in order to make certain that the patient does not experience a “pinching” sensation, and then the band is deployed. A post-banding rectal exam is then performed in order to confirm placement of the band, as well as to manipulate the band if required for patient comfort. Analgesics are not required, and the patient is free to return to work after the procedure. It is recommended that a single column be treated at a setting in order to minimize complications and avoid the use of analgesics9, as well as to allow the patient to return to full activities immediately. Dr. Iain Cleator has reported on the largest series of patients utilizing this technology, reporting a 99% success rate with less than a 1% complication rate and a recurrence rate of only 5% at two years6. The typical patient requires a series of three treatments, and the patient can typically return to work immediately. There is no sedation, prep or other pre-procedure requirements other than discontinuing anticoagulants such as Warfarin or Clopidogrel. CRH Medical Corporation has developed a comprehensive educational and support program in order to help introduce this technology. This program, led by board-certified physicians (who are experts in this technology), includes a didactic presentation reviewing the medical management of hemorrhoids, anal fissures and other ano-rectal disorders, followed by “hands-on” instruction in RBL techniques. A similar program is offered for fellowship training programs, along with the availability of “Grand Rounds” type lectures, all at no cost to the trainee/department. Follow-up training sessions are also offered and, in fact, encouraged. Physician-based support and consultative assistance are also provided in a “24/7” format.
PATIENT SELECTION AND TREATMENT INDICATIONS
Patients tend to present with one or more of several symptoms, including rectal bleeding, peri-anal itching, prolapsing tissue and/or associated discomfort. RBL has been shown to be beneficial in the vast majority of Grades I–III hemorrhoids and in a significant number of Grade IV patients. (Several methods of converting a Grade IV patient back to a Grade II or III may be employed in order to make these patients candidates for RBL.) Too often patients are evaluated for rectal bleeding or other symptoms, and then told after an otherwise negative colonoscopic exam that hemorrhoids are the cause of their symptoms, only to be dismissed even after the failure of conservative medical treatment. “If a colonoscopy is performed for recurrent rectal bleeding or occult blood, and the solitary finding of internal hemorrhoids is noted and felt to be the cause of this bleeding, the gastroenterologist should feel compelled to initiate effective treatment (RBL) for the patient,” states Dr. Robert Gannan, MD, PhD. “This is vital in order to eliminate that bleeding, and so potentially confuse our ability to follow these patients, as well as to help avoid a premature and otherwise unnecessary colonoscopy7.”
Figure 2 CRH Technique using “touch” technique. Courtesy Iain Cleator, MD.
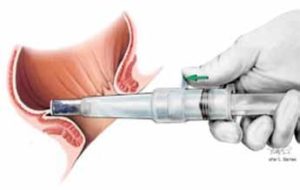
Figure 3 Technique using paired slotted anoscope. Courtesy Iain Cleator, MD.
EFFICACY OF TREATMENT: “CASE STUDY” OF ADOPTION WITHIN THE GI PRACTICE
The first large GI group to incorporate the CRH O’Regan System™ into their practice was the Atlanta Gastroenterology Associates group in metropolitan Atlanta, GA. Dr. Neal Osborn, MD, MSc, reported the group’s early experience at the 2009 DDW8, as 11 gastroenterologists treated 113 patients by way of 257 banding events. Their initial experience led to resolution of the pre-banding symptoms in 94% of patients, and a delayed success rate of over 80% of the patients by three months. There were few minor complications noted, and only one patient (0.8%) with bleeding requiring the GI’s further input. Notably, this level of success, with so few complications, was noted at the onset of the group’s experience.
“LEARNING CURVE”
The report from Dr. Osborn (Atlanta Gastroenterology) indicated the lack of a “learning curve,” and these findings have been reinforced by the feedback received from many of the approximately 400 physicians that have been trained by CRH prior to adopting these techniques. It is expected that, with additional experience, these clinicians’ results will even more closely resemble those of Dr. Cleator.
START-UP COSTS
As the CRH O’Regan System™ requires no special equipment, there are no capital costs for ancillary equipment. The kit supplied is all inclusive of the device elements needed. Specifically, in contrast to other hemorrhoidal banding techniques that require endoscopy, there are no ancillary costs for use, upkeep and depreciation of endoscopes.
INCORPORATION INTO A GI PRACTICE: SCHEDULING RATIONALE
Most gastroenterology practices schedule these cases at 5-10 minute intervals per patient. This allows adequate time for the procedure and evaluation of the patient prior to discharge. These procedures can be done in an ASC or in the office, although the total reimbursement, professional and facility, is higher for procedures performed in the ASC. Because of the fact that these patients are not “NPO,” they are prime candidates to be scheduled later in the day at the ASC, when excess capacity often is present, making this a perfect complement to the “case mix” performed within the center. In contrast to colonoscopy scheduling where the procedure time blocked for each room is typically 30 minutes (2/hour) for one case, 5-6 hemorrhoidal bandings can be booked during that same hour timeframe. The implications for a patient cancellation or “no show” are obviously far more favorable for the efficient and profitable use of the facility. Furthermore, hemorrhoidal banding time is predictably short for each procedure, whereas time for colonoscopy is relatively unpredictable. The implications for prolonged colonoscopy and schedule disruptions are well known to gastroenterologists…and the GI nurses!
REVENUE
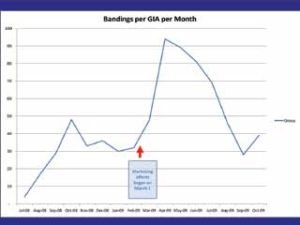
Safe and effective treatment is clearly the prime focus for any interventions made in patient care. The business case for the use of the CRH O’Regan band ligator, however, has strikingly favorable implications for incorporation to standard practice of gastroenterologists. Current third party reimbursement provides revenue that not only covers overhead costs, but according to Bergein F. Overholt, MD, of Gastrointestinal Associates, Knoxville, TN, “produces a ‘revenue per minute’ for the physician and the ASC that is equal to or greater than other services gastroenterologists provide. RBL using the O’Regan device has allowed our group to improve patient care and at the same time has significantly improved our practice and ASC revenues.” Most gastroenterologists perform RBL on patients within their own practices or on those referred by other physicians. Yet RBL is a successful technique that can and will bring new patients to the practice for banding once patients become aware of a safe, effective and painless method of treating hemorrhoids. Many of those patients will also have other GI problems that require care (including colonoscopy), creating a long-term patient relationship. Marketing the procedure to the public is one way to create the awareness of a safe, effective and essentially painless treatment for hemorrhoids and to bring patients to the practice. One practice used newspaper media marketing resulting in a large increase in patients seen for the O’Regan banding (fig. 4). The response was so dramatic that the practice is developing a periodic marketing program throughout the year. Every physician that is trained by CRH also has the opportunity to be listed on CRH’s industry leading website www.www.oregansystem.com. Many physicians on this website report a significant number of new patients as a result.
Figure 4
Impact of initial marketing campaign on number of procedures performed using CRH O’Regan System™
CONCLUSION
There is significant patient need for care of symptomatic hemorrhoids unresponsive to medical measures. RBL provides a simple, safe, effective means of treating these patients, and CRH Medical Products Corporation offers a comprehensive training and support program to aid the incorporation of these techniques utilizing the CRH O’Regan System™. This program affords the GI physician the ability to provide more comprehensive care to their patients, benefitting both the patient and their practice.
1. Practice Parameters for the Management of Hemorrhoids (revised). Dis Colon Rectum. 2005 Feb; 48(2):189-94. Cataldo P
2. Prevalence of Major Digestive Disorders and Bowel Symptoms, 1989. Adv Data. LeClere FB, Moss A, Everhart JE, Roth HP.
3. Definitive Therapy for Internal Hemorrhoids – New Opportunities and Options. Rev Gastroenterol Disord. 2009; 9 (1): 16-26. Ohning GV, Machicado GA, Jensen DM.
4. Hemorrhoids. Surg Clin N Am 2002; 82:1153-1167. Sardinha TC, Corman ML.
5. Hemorrhoids. In: Corman ML, editor. Colon and rectal surgery. 4th edition. 1998:147-205. Philadelphia: Lippincott-Raven. Corman ML
6. Banding Hemorrhoids Using the O’Regan Disposable Bander. Business Briefings. US Gastroenterol Rev. 2005:69-73. Cleator IGM, Cleator MM.
7. Personal Correspondence, Robert Gannan, MD, PhD, Dec, 2009.
8. Hemorrhoid Treatment in the Outpatient Gastroenterology Practice Using the O’Regan Disposable Hemorrhoid Banding System is Safe and Effective. J Med. 2009; 2 (5):248-256. Osborn NK, King KH, Adeniji OA, et. al.
9. Multiple Hemorrhoidal Bandings in a Single Session. Dis Colon Rectum 1994 Jan; 37(1):37-41. Lee HH, Spencer RJ, Beart RW, Jr.
Mitchel Guttenplan, MD, FACS, practices at the Center for Colorectal Health in Atlanta, GA. He is board certified in surgery after graduating from Emory University Medical School and completing his surgical residency at the Emory University Affiliated Hospitals. He is also a Fellow of the American College of Surgeons as well as the Medical Director of CRH Medical. Dr. Guttenplan has been very active in helping to train gastroenterologists in the care of anorectal disorders, and has been a guest lecturer at numerous GI meetings, hospitals and GI fellowship programs. For more information, please email him at mguttenplan@crhmedcorp.com.
David A. Johnson, MD, FACP, FACG, FASGE, is Professor of Medicine and Chief of Gastroenterology
at Eastern Virginia School of Medicine. He has published extensively in the internal medicine and gastroenterology literature, contributing over 350 articles, chapters, or abstracts to peer-reviewed journals. He has been involved extensively in committees of the national GI societies and is the immediate Past President
of The American College of Gastroenterology. He is co-editor of Reviews in Gastroenterologic Disorders and is section editor for the Medscape Gastroenterology Viewpoints series as well as Journal Watch Gastroenterology (from the publishers of The New England Journal of Medicine). He is on numerous editorial boards and serves as a reviewer for 18 medical journals, including all of the gastroenterology journals as well as a number of prestigious internal medicine journals, such as Annals of Internal Medicine, Archives of Internal Medicine, The American Journal of Medicine, and The Lancet. He is coeditor of the American College of Physicians book Dyspepsia and editor of the 2005 Gastroenterology Clinics of North America issue “Obesity and the Gastroenterologist.”
Bergein F. Overholt, MD, MACG, FACP, FASGE, has served as President of Gasstrointestinal Associates, P.C. and as medical director of The Endoscopy Center, Knoxville, Tennessee. He is medical
director of the Laser Center of the Thompson Cancer Survival Center in Knoxville. Dr. Overholt is a past president of the American Society for Gastrointestinal Endoscopy. He is a past board member and medical director of AmSurg.